Call center quality assurance in healthcare is the practice of scoring patient phone interactions against defined criteria for compliance, accuracy, and communication. Most programs have a blind spot: if your team manually reviews 1 to 5 percent of patient calls, the other 95 to 99 percent go unmonitored, carrying unexamined compliance risk, missed coaching opportunities, and hidden patient experience gaps.
For healthcare operations leaders managing healthcare call center teams, this gap is not just a performance issue. It is a regulatory liability. Every unreviewed call where an agent mishandles PHI, skips an identity verification step, or provides inaccurate insurance guidance is a potential HIPAA violation that your current QA process cannot catch.
This guide walks you through a five-step framework for building a QA program that covers 100% of calls, automates compliance monitoring, and creates the audit trails your organization needs.
What You'll Need Before You Start
Before restructuring your QA program, gather these baseline components:
- Current QA scorecards and evaluation criteria: you will rebuild these, but understanding your starting point matters
- Call volume data from the past 90 days, segmented by call type (scheduling, billing, referrals, prescription inquiries)
- Compliance incident history: any documented HIPAA violations, patient complaints, or audit findings
- Agent performance data including quality scores, first call resolution rates, and average handle times
- Technology inventory: your current recording platform, EHR systems (Epic, athenahealth, eClinicalWorks, or NextGen), and any analytics tools already in place
- Stakeholder alignment from compliance, operations, and IT leadership on QA program goals
Step 1: Audit Your Current QA Baseline
Most QA overhauls fail because teams jump straight to new tools without understanding where their current program breaks down. Start with an honest assessment.
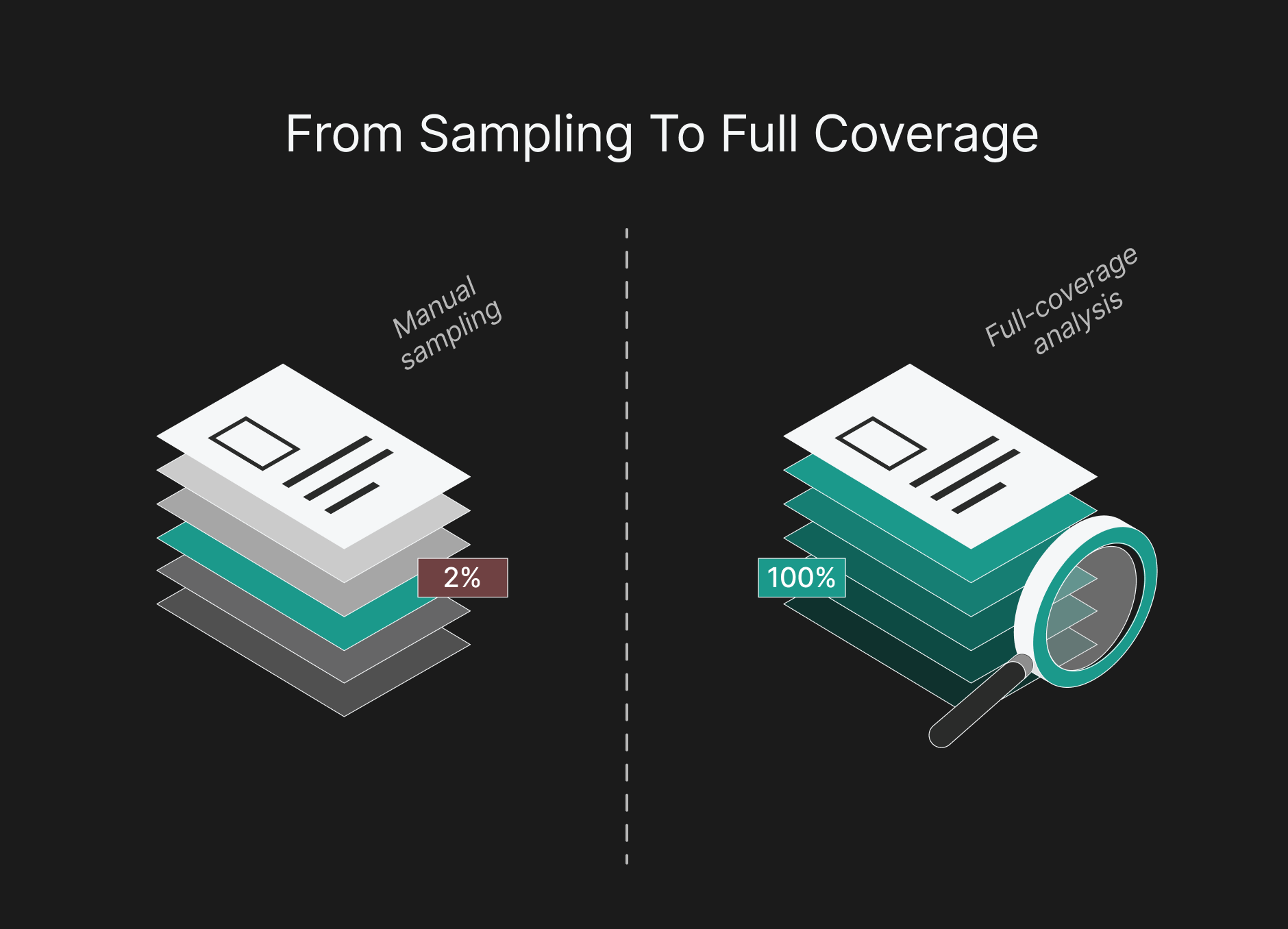
Quantify your coverage gap. Calculate the percentage of calls reviewed each month. If you handle 10,000 calls and score 200, that is 2% coverage. Document this number as your benchmark.
Map your risk exposure. Categorize the unreviewed 98% by call type and risk level. Prescription calls carry more compliance risk than appointment confirmations. Billing calls involving insurance may require PCI-DSS adherence alongside HIPAA. Not all unmonitored calls carry equal risk.
Assess scorecard relevance. Many healthcare call centers use generic QA scorecards from retail or telecom. Check whether your criteria include healthcare-specific compliance checkpoints:
- Two-factor patient identity verification before any PHI is discussed
- A call recording disclosure delivered early in the call
- Correct handling of eligibility and benefits questions, including the 270/271 response
- Accurate explanation of patient financial responsibility on billing calls
- Escalation and documentation steps for clinical triage calls
If more than two items are missing, your scorecard needs a healthcare-specific rebuild.
Step 2: Build Healthcare-Specific Scorecards
Generic scorecards fail in healthcare because scheduling calls and billing disputes require different evaluation criteria. Build separate scorecards for each call type, with shared compliance elements across all.
Shared compliance layer (all call types):
- Patient identity verified using two-factor authentication (name + DOB, or name + MRN)
- Call recording disclosure delivered within first 15 seconds
- PHI discussed only after identity confirmation
- No unauthorized disclosure of patient information to third parties
Call-type-specific criteria examples:
For scheduling calls, weight accuracy (correct provider, correct location, correct time slot) and patient communication (appointment prep instructions, cancellation policy).
For billing and insurance calls, weight eligibility verification accuracy, correct explanation of patient financial responsibility, and handling of payment card information.
For clinical triage calls, weight adherence to nurse triage protocols, appropriate urgency escalation, and documentation completeness.
Scoring structure recommendation: Use a weighted model where compliance elements account for 40% of the total score, accuracy for 30%, and patient communication for 30%. This ensures compliance failures surface, even when an agent scores well on soft skills.
See where an AI agent fits in your operation.
Book a demoStep 3: Move from Sampling to Full-Coverage Analysis
The contact center quality assurance software market is growing from $2.25 billion in 2025 to $4.09 billion by 2032, driven largely by AI-powered tools that enable 100% call analysis. This is the most significant shift in QA methodology available to healthcare operations teams today.
Why sampling fails in healthcare. In a 2% sample, a single agent’s HIPAA violation has a 98% chance of going undetected in a given month. Across 50 agents handling complex patient calls, that compliance exposure becomes significant. For regulated industries, sampling is not a quality strategy. It is risk acceptance.
How voice analytics in healthcare works. AI-powered platforms transcribe and analyze calls in real time, scoring against your custom scorecards automatically. The technology detects:
- SOP adherence: did the agent follow the required verification steps in the correct order?
- Sentiment shifts: did the patient's tone indicate frustration, confusion, or distress?
- Compliance triggers: was PHI disclosed before identity verification? Were required disclosures missed?
- Topic classification: what was the call actually about, and was it routed correctly?
Platforms like Flexbone's Voice Room analyze 100% of calls and apply automated SOP scoring, giving QA teams complete visibility rather than statistical guesses. When evaluating healthcare call center software, prioritize solutions that offer full-coverage analysis over those that simply digitize the sampling process.
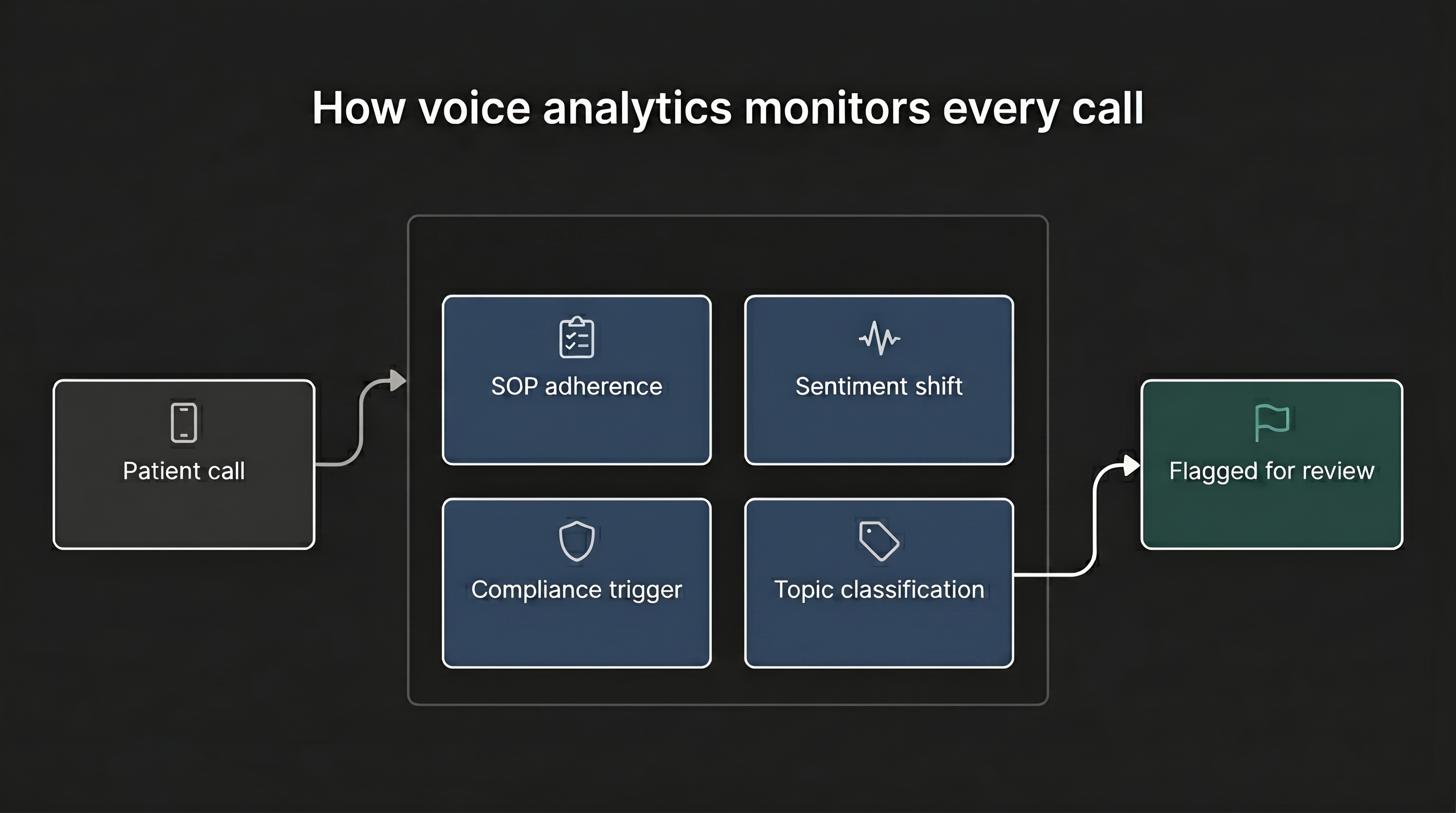
The human reviewer's new role. AI does not replace QA analysts. It redirects them. Instead of reviewing random calls, your team focuses on flagged interactions that need human judgment, such as complex escalations, unclear compliance situations, and coaching opportunities AI can identify but not resolve.
Step 4: Automate Compliance Monitoring and Audit Trails
The HIPAA Security Rule requires covered entities to retain required documentation for six years, and to record who accessed PHI, when, and what actions they took. Your QA program should generate these records automatically, not retroactively.
Build continuous compliance monitoring. Configure your QA platform to flag compliance deviations in real time, not in weekly reports. If an agent skips identity verification before discussing lab results, the system should send an immediate alert and create a documented record.
Automate audit trail generation. Every QA evaluation, whether AI-generated or human-completed, should produce a timestamped, immutable record that includes:
- Call ID and timestamp
- Agent identifier
- Scorecard version used
- Individual criterion scores with pass/fail flags
- Compliance deviation details (if any)
- Reviewer identity (human or AI system)
- Follow-up actions taken
Zero-retention architecture matters. In healthcare, the QA platform can become a PHI liability. Zero-retention solutions, like Flexbone’s approach, analyze calls in real time without permanently storing raw audio with patient data. This reduces compliance risk while still producing scored records and audit trails.
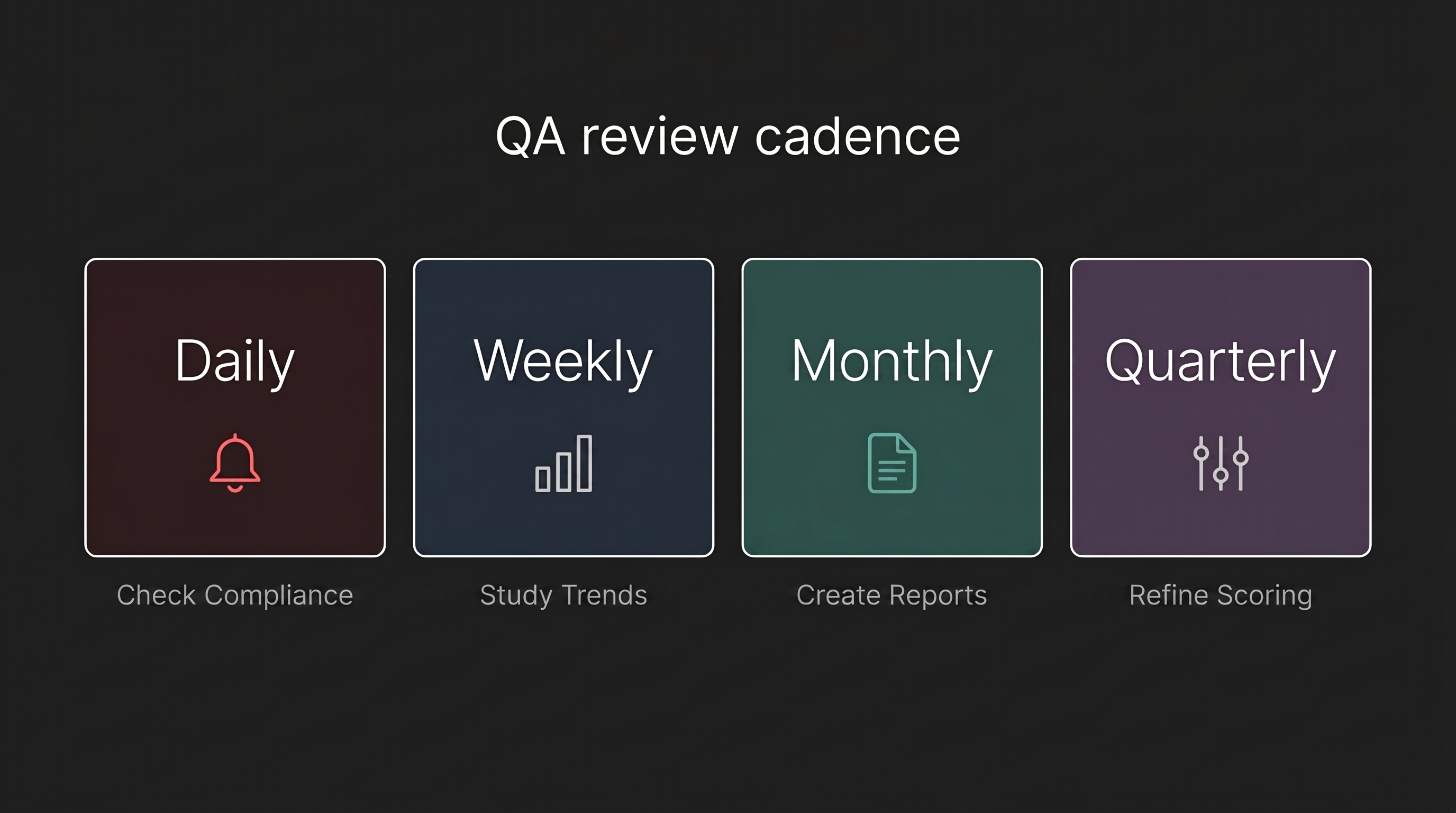
Establish review cadences. Automated monitoring generates data. You need structured processes to act on it:
- Daily: Review AI-flagged compliance deviations (target: same-day response)
- Weekly: Analyze agent performance trends and identify coaching priorities
- Monthly: Generate compliance summary reports for leadership
Quarterly: Calibrate AI scoring against human reviewer scores to ensure alignment
Step 5: Connect QA Data to Operational Outcomes
QA data becomes more powerful when connected to the metrics your organization already tracks. Isolated quality scores only show how agents perform on calls. Connected QA data tells you how call quality affects patient satisfaction, revenue, and operational efficiency.
- Link QA scores to first call resolution: When agents consistently score high on accuracy and protocol adherence, first call resolution rates improve because patients get correct information the first time. Track the correlation between QA scores and FCR at the agent level to identify where coaching investments yield the highest returns. Healthcare call centers typically benchmark FCR at 75-85% .
- Measure downstream revenue impact: Track how QA improvements affect scheduling completion, insurance verification accuracy, and billing dispute resolution. Comprehensive call analysis can help recover revenue lost to scheduling errors and eligibility verification mistakes.
- Feed QA insights into training programs: Aggregate QA data reveals patterns individual call reviews miss. If 30% of billing calls score low on explanation clarity, the issue may be a training gap or process design problem. Use QA trends to build targeted training instead of generic refreshers.
Troubleshooting Common QA Program Issues
- Agent resistance to AI monitoring: Frame AI-powered QA as a fairness improvement, not surveillance. With sampling, an agent may be judged on only 3-4 calls per month. With full-coverage analysis, scores reflect all interactions, making them more representative. Involve agents in scorecard design and show scores in real time.
- Score calibration drift: Over time, AI and human scoring can diverge. Hold monthly calibration sessions where reviewers score calls independently, then compare results with AI scores. Adjust the model when the gap exceeds 5%.
- Data overload: Moving from 200 reviewed calls to 10,000 analyzed calls per month creates far more data. Use exception-based workflows so your team only reviews calls that deviate from expected performance, not the calls that meet standards.
- EHR integration challenges: Connecting QA data to patient outcomes requires EHR integration. Evaluate platforms by integration depth. Flexbone, for example, integrates with 15+ EHR systems, including Epic, athenahealth, eClinicalWorks, and NextGen, so QA data can support existing clinical and operational workflows.