
First call resolution (FCR) in healthcare is the share of patient inquiries fully resolved on the first interaction, with no follow-up needed. The industry average is about 71 percent, according to SQM Group benchmarking, which means roughly three in ten callers have to call back. Nearly 29 percent of patient calls to healthcare organizations require at least one callback, and each repeat contact adds operational cost, strains agent capacity, and weakens the trust patients place in your organization.
This guide walks you through seven practical steps to improve healthcare FCR performance and move closer to the top-tier benchmark of 80 percent or higher. Whether you manage a health plan member services team or a hospital patient access center, these strategies are built for the operational challenges you face every day. For the broader picture, see our healthcare call center optimization guide.
Why First Call Resolution Matters More in Healthcare
Before diving into the steps, it helps to understand why FCR deserves your focused attention over other metrics.
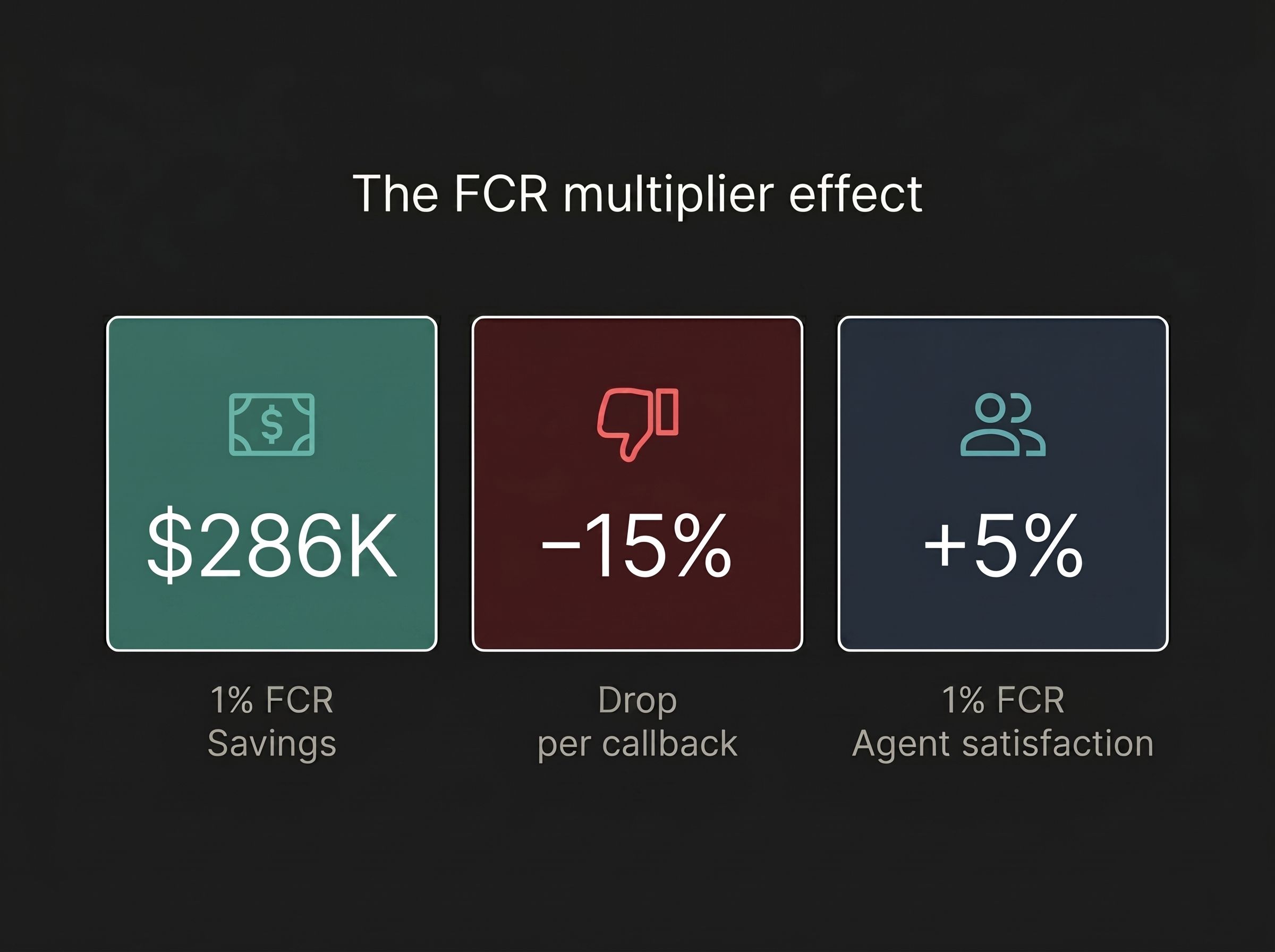
Financial impact. For the average healthcare call center, a 1% improvement in FCR equals approximately $286,000 in annual operational savings, according to SQM Group. That number comes primarily from eliminating repeat calls and the agent time they consume.
Patient satisfaction. FCR has the highest correlation to satisfaction of any call center metric. SQM's research shows that satisfaction drops 15% on average every time a patient or member has to call back. If you want to improve your CSAT score, FCR is the single most effective lever you can pull. The relationship between call resolution and patient satisfaction is direct and well-documented.
Agent retention. For every 1% improvement in FCR, employee satisfaction improves by up to 5%. Agents handling repeat calls from frustrated patients face higher stress levels and burn out faster. In an industry where call center agent turnover runs 40% to 45% annually, protecting your team matters.
Healthcare complexity. Unlike retail or tech support, healthcare calls often involve anxious patients dealing with benefits, authorizations, prescriptions, and appointments. The stakes are personal, so unresolved calls cause damage.
What You'll Need Before You Start
Before working through the steps below, make sure you have:
- A baseline FCR measurement: You cannot improve what you have not measured. If you do not have FCR data yet, Step 1 covers this.
- Call recording or QA infrastructure: You need a way to review calls and spot patterns. Even basic call recording is enough to start.
- Access to repeat-call data: Your phone system or CRM should show when the same patient calls more than once within a set window, usually 7 to 14 days.
Common mistake to avoid: Do not rely only on agent self-reporting to track FCR. Agents often overestimate resolution rates, while VoC surveys usually provide more accurate results.
Step 1: Measure FCR Accurately (Stop Relying on Guesswork)
The first step is establishing a reliable FCR measurement system.
The formula is straightforward:
(Number of issues resolved on first call / Total number of patient calls) x 100 = FCR Rate %
For example, if your team handled 4,000 patient calls last month and 2,840 were resolved without a follow-up contact, your FCR rate is 71%.
The measurement method matters as much as the formula. There are two primary approaches:
SQM Group recommends using VoC post-call surveys as the gold standard. The patient is the one who determines whether their question was truly answered.
You also need two internal definitions before measurement begins:
- What counts as "resolved": Did the patient get a complete answer, or just a partial one?
- What is your callback window? If a patient calls back about the same issue within 7 days (or 14, depending on your policy), that original call was not resolved.
Establishing solid measurement is also the foundation for effective call center quality assurance, since FCR data tells you exactly where your QA efforts should focus.
Common mistake to avoid: Do not measure FCR without clearly defining what “same issue” means. A billing call followed by an appointment call is not a repeat call, so be precise.
Step 2: Identify Your Top Repeat-Call Drivers
Once you can measure FCR, the next step is figuring out why patients are calling back. Not all repeat calls have the same root cause, so focus first on the highest-volume drivers.
Categorize your repeat calls by type. In most healthcare organizations, the breakdown looks something like this:
Run a root cause analysis on your top two or three categories. Techniques like the “5 Whys” method work well here. For example:
- Why did the patient call back? Their eligibility was not confirmed.
- Why was eligibility not confirmed? The agent could not access real-time insurance data.
- Why not? The insurance verification system is not integrated with the call platform.
- Root cause: System integration gap, not agent performance.
Training alone will not fix problems caused by missing data or disconnected systems.
Step 3: Build a Knowledge Base That Agents Actually Use
A comprehensive knowledge base is one of the most cost-effective tools for improving FCR. But “comprehensive” does not mean dumping every document into a shared drive.
Structure it by call type, not by department. When a patient calls about eligibility, agents should not have to search across billing, enrollment, or payer relations folders. Organize content around the questions patients actually ask.
Include payer-specific guides. Healthcare is complex because each payer has different rules. Your knowledge base should include per-payer guides for eligibility checks, prior authorization requirements, denial codes (the CARC and RARC codes returned on remittances), and appeals.
Keep it current. A knowledge base last updated six months ago can lead to wrong answers. Assign ownership and review it monthly, especially during open enrollment when payer rules change.
Common mistake to avoid: Building a knowledge base and calling it “done” is a mistake. The best knowledge bases are living documents, updated weekly based on new repeat-call patterns from Step 2.
Step 4: Train Agents on Healthcare-Specific Scenarios
Generic customer service training does not fully prepare agents for healthcare calls. Patients asking about denials, authorization delays, or confusing bills need agents who understand both the process and the emotional weight involved.
- Use scenario-based role-plays: Build training around the call types driving repeat calls. If eligibility verification is the top driver, spend most of your training time there.
- Train soft skills alongside process skills: Healthcare callers are often stressed, confused, or in pain. Agents need to show empathy while moving efficiently toward resolution. These goals work together. For example: “I understand this is frustrating. Let me pull up your coverage so we can sort this out together.”
- Use real call recordings: Use examples of both high-FCR and low-FCR calls. Let agents identify what high-performing agents did differently. This peer-learning approach is often more effective than lectures.
Common mistake to avoid: Do not train only new hires. Experienced agents also develop habits that need coaching. Quarterly refresher sessions tied to repeat-call data help keep the whole team sharp.
See where an AI agent fits in your operation.
Book a demoStep 5: Integrate Systems to Eliminate Information Silos
Many FCR failures are not caused by undertrained agents. They happen because agents cannot access the information they need during a live call. When agents switch between multiple screens, place patients on hold, or promise a callback, the root cause is often a systems problem.
EHR integration. Agents should see key patient details, such as demographics, recent visits, care team, and active orders, without leaving the call platform. Integrated access to EHRs like Epic or athenahealth helps resolve calls faster and more completely, and it keeps that data flow inside a HIPAA-compliant boundary.
Real-time insurance verification. Instead of manually checking payer portals, agents can use integrated tools to run a 270/271 eligibility transaction and confirm coverage during the call.
Scheduling system access. If an agent cannot see real-time appointment availability, they cannot schedule during the call. That becomes a callback.
Unified interaction history. When a patient calls back, the next agent should see the full record of the previous interaction. CRM integration prevents patients from repeating their story.
System integration also has a direct impact on average handle time. When agents have the data they need at their fingertips, calls are both shorter and more likely to reach resolution.
Common mistake to avoid: Do not buy “integrated” software that still requires separate logins. True integration means one view for patient, insurance, scheduling, and interaction data.
Step 6: Deploy AI-Powered Call Analysis for Full Visibility
Traditional QA in healthcare call centers often relies on supervisors reviewing just 1% to 5% of calls. That means 95% or more go unreviewed, and FCR decisions are based on only a small slice of your data.
AI-powered call analysis platforms change this by analyzing 100% of calls automatically. These platforms use natural language processing to:
- Identify repeat-call patterns that manual review would miss
- Detect sentiment shifts that signal unresolved issues (e.g., a patient who starts the call calm but ends frustrated)
- Flag specific call types with low resolution rates for targeted intervention
- Surface coaching opportunities for individual agents based on actual call performance
Platforms like Flexbone’s Voice Room and others provide full-coverage analysis that turns patient interactions into usable data. Instead of guessing which calls to review, you get a clearer picture of where FCR is failing and why.
This shift from sampling to full-coverage analysis is especially useful in healthcare FCR improvement because calls vary widely. A 3% sample may miss eligibility verification calls while over-representing routine appointment confirmations.
Common mistake to avoid: Treating AI call analysis as a replacement for human QA reviewers is a mistake. The technology identifies patterns and flags issues at scale, but supervisors still need to review calls, coach agents, and make process decisions.
Step 7: Automate Eligibility Verification to Prevent Callbacks
Insurance eligibility and prior authorization errors are among the most common and preventable drivers of repeat calls in healthcare. When coverage status is unclear, incorrect, or unverified during the call, a callback is routinely needed. Prior authorization compounds the problem: physicians and their staff spend an average of 13 hours a week on it, per AMA survey data, and an unresolved auth is a frequent reason a patient calls back.
Automate verification at two points:
- At scheduling: When a patient books an appointment, an automated eligibility check confirms coverage, copay, and any requirements such as prior authorization or referral. Issues are flagged before the visit.
- Day-of-appointment: A second automated check catches coverage changes between scheduling and the visit date.
This two-pass approach helps prevent repeat calls, billing confusion, and claim denials. Some healthcare organizations report recovering about $80,000 per month by reducing eligibility errors and rework.
Common mistake to avoid: Automating eligibility verification without updating results in the call platform. If agents cannot see the verification status during a live call, automation adds a step without solving the problem.
Troubleshooting: When FCR Improvements Stall
Even with the right strategy, you may hit plateaus. Here are three common scenarios and how to address them:
FCR is improving but AHT is spiking. Agents may be over-explaining or spending too long on calls to ensure resolution. Use more concise knowledge base answers and decision trees to guide faster resolutions.
FCR is flat despite heavy training investment. Repeat-call drivers may be systemic, not agent-related. Revisit Step 2 to see whether process or system issues are the real cause.
Agents appear to be gaming the metric. If agents mark calls as resolved while patients still call back, switch to VoC post-call surveys. Let the patient be the judge.
Your 30/60/90-Day FCR Improvement Roadmap
Improving FCR healthcare performance is not a one-time project. It is a system you build over time. Here is how to sequence the work:
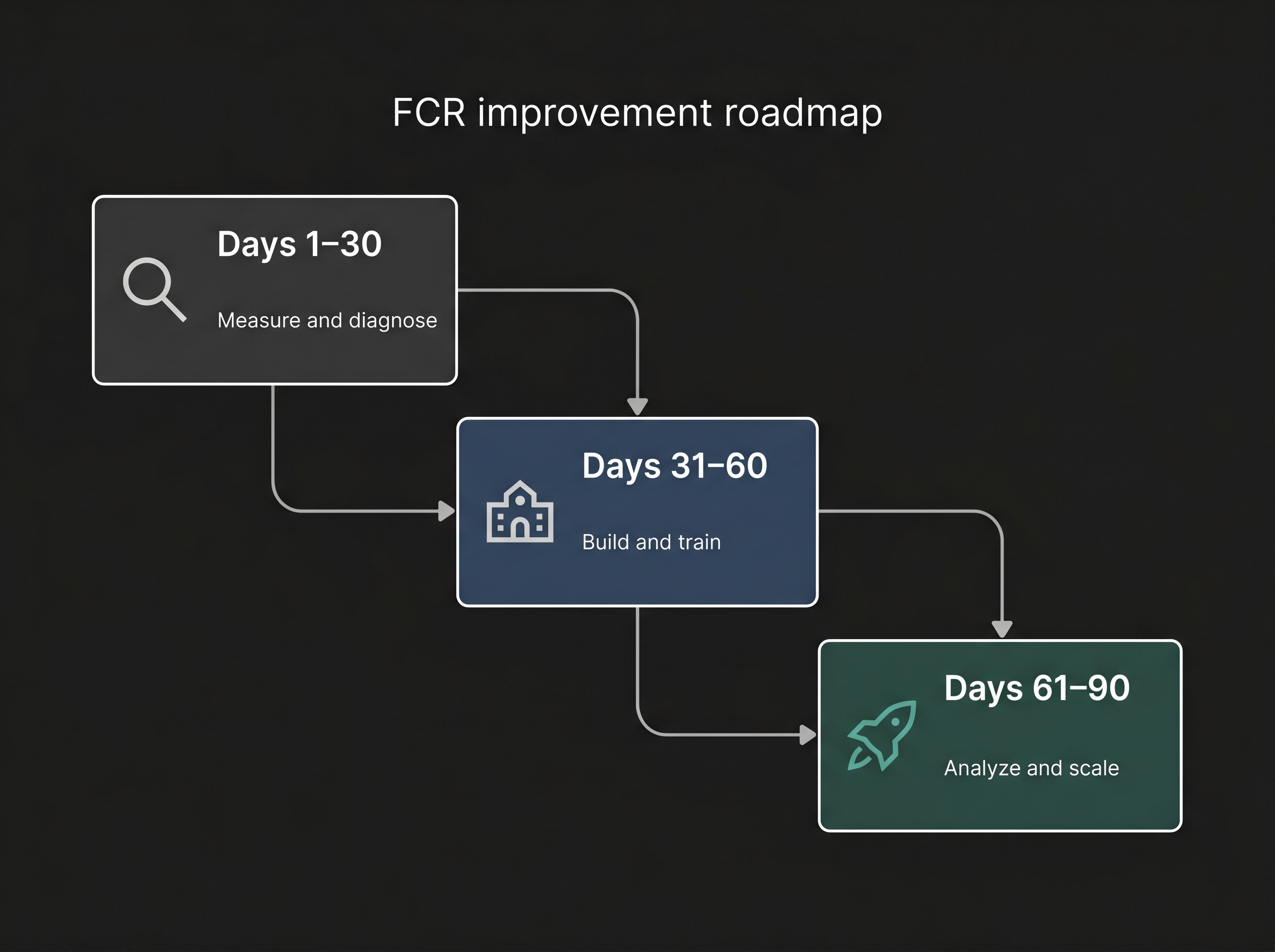
Days 1-30: Measure and Diagnose
- Implement VoC post-call surveys to establish your true FCR baseline
- Pull repeat-call data and categorize the top three drivers
- Audit your current knowledge base for gaps and outdated content
Days 31-60: Build and Train
- Restructure your knowledge base around call types (not departments)
- Launch scenario-based training focused on your top repeat-call categories
- Begin system integration work (EHR, insurance verification, scheduling)
Days 61-90: Analyze and Scale
- Deploy AI-powered call analysis to move from sampling to full-coverage review
- Automate eligibility verification at scheduling and day-of-appointment
- Set a monthly FCR review cadence and benchmark against the 80%+ top-tier standard
Healthcare organizations that implement VoC FCR measurement can expect an average improvement of 3% or better, and in most cases, meaningful improvement takes place within 90 days.
The steps in this guide work together. Measurement without root cause analysis creates data you cannot act on. Training without system integration leaves agents without the right tools. Technology without training creates expensive tools no one uses effectively.
Start with Step 1 and work through them in order. For a complete framework covering FCR alongside AHT, CSAT, QA, and other critical metrics, read our healthcare call center optimization guide.