If you are evaluating medical call center solutions right now, you are not alone. The healthcare CCaaS market hit $7.05 billion in 2025 and is growing at 20.34% annually, driven by a simple reality: patients expect more, staff capacity is shrinking, and the gap between what is possible and what most health systems actually run is widening fast.
This guide is for operations leaders, IT directors, and practice administrators who need to make a confident purchasing decision. We cover the evaluation criteria that matter, pricing models you will encounter, implementation traps to avoid, and red flags that should send you elsewhere. Whether you run a 50-bed community hospital or a multi-state health system, this framework applies. The pressure behind the decision is documented: MGMA reports that phone volume remains a backlog that costs medical practices time they cannot easily staff for.
What Is a Medical Call Center (and Why It Matters in 2026)?
A medical call center is the centralized communication hub where patients interact with your organization by phone, chat, SMS, or video to schedule appointments, address billing questions, request prescription refills, obtain referrals, receive triage, and follow up on care. It is not the front desk or a generic answering service. It is a clinical operations function that directly shapes patient access, revenue capture, and satisfaction scores.
The distinction matters because general-purpose contact center software was not built for healthcare workflows. A hospital call center handles protected health information on every interaction, routes calls by clinical acuity, and needs to pull and push EHR data in real time. Generic platforms bolt on HIPAA compliance as an afterthought. Purpose-built solutions start there.
In 2026, three forces are reshaping what "good" looks like:
- AI is now common, not a differentiator. A large share of healthcare call center leaders are deploying or planning to deploy large language model solutions. If your current vendor does not have a concrete AI roadmap, you are behind the field.
- Staffing pressure is structural. The Health Resources and Services Administration projects ongoing shortages in clinical and administrative roles. Your patient call center strategy needs to do more with fewer people, not just fill seats.
- Patient expectations have shifted permanently. Difficulty reaching a provider is one of the most common barriers patients cite to good healthcare communication. Hold times, abandoned calls, and callback failures are not operational inconveniences; they are access-of-care problems.
Key Features to Evaluate in a Medical Call Center Solution
Not every feature matters equally. The five categories below separate solutions that work from solutions that create new problems.
EHR and Clinical System Integration
This is the most important capability to evaluate. If your medical call center platform cannot read from and write to your EHR in real time, agents are toggling between systems, manually entering data, and introducing errors as they go.
Look for:
- Bidirectional EHR integration (not just read access). Agents should be able to schedule, update demographics, and document interactions directly from the call center interface.
- Support for your specific EHR: "We integrate with EHRs" is not the same as "We have a production-validated integration with Epic, Cerner, or athenahealth." Ask for customer references running your exact stack.
- HL7 FHIR support: The FHIR standard is becoming the baseline for interoperability. Solutions that rely solely on proprietary connectors create long-term lock-in risk.
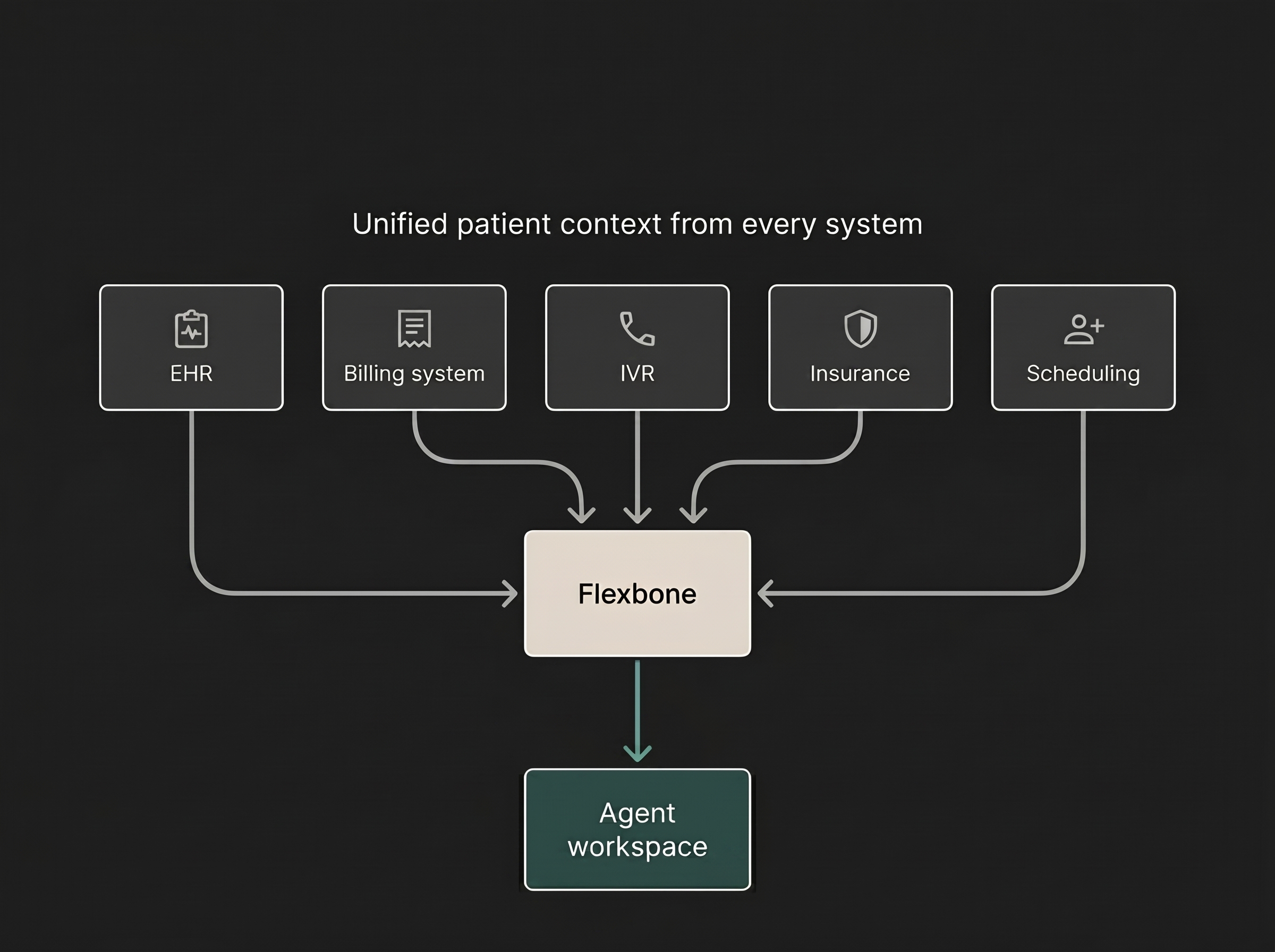
- CRM and billing system connectivity: The best healthcare call center software unifies patient context across clinical, financial, and operational systems so agents resolve issues on the first call instead of transferring.
Some platforms, like Flexbone AI, offer 15+ validated EHR integrations out of the box. Others require months of custom development. The gap between “we can integrate” and “we have integrated” is often six figures and six months.
AI-Powered Automation and Intelligent Routing
AI in a patient call center is not about replacing agents. It is about handling the 40-60% of predictable interactions, like appointment scheduling, prescription refills, insurance verification, and balance inquiries, so trained staff can focus on complex clinical and billing calls.
Evaluate these capabilities:
- Conversational AI agents that complete transactions end-to-end, not just collect information and hand off. Can the AI book an appointment in your scheduling system, or just take a message?
- Intelligent call routing based on clinical context, not just menu selections. Skills-based routing that accounts for call type, patient acuity, insurance, and agent specialization reduces transfers and improves first call resolution.
- Agent assist tools that surface relevant information during live calls: patient history, prior interactions, insurance eligibility, and suggested responses. This is where AI augments human performance rather than replacing it.
- Predictive analytics for staffing and volume forecasting. AI should help you schedule the right number of agents before call spikes, not just report on them after.
Compliance, Security, and Data Governance
Every medical call center vendor will tell you they are HIPAA-compliant. The question is how deep that compliance runs.
Go beyond the checkbox:
- BAA (Business Associate Agreement) signed and current. This is not optional. If a vendor hesitates, walk away.
- Encryption at rest and in transit for all patient data, call recordings, and chat transcripts.
- Access controls with role-based permissions, audit trails, and automatic session timeouts.
- Data retention policies that align with your state's requirements (which often exceed federal minimums).
- Zero-retention options: Some platforms now process patient data without storing it on the vendor’s infrastructure, eliminating an entire category of breach risk.
- SOC 2 Type II and HITRUST certifications: SOC 2 is the baseline. HITRUST is the gold standard for healthcare.
For a deeper look at how compliance intersects with broader healthcare call center optimization, see our pillar guide.
Analytics, QA, and Performance Reporting
You cannot improve what you cannot measure. Your medical call center analytics determine whether you manage by anecdote or by data.
Critical capabilities:
- 100% call analysis vs. sampling: Most legacy QA programs review 1-5% of calls. Modern AI-powered platforms can analyze every interaction for sentiment, compliance, script accuracy, and outcome. The difference between sampling and census-level analysis is the difference between guessing and knowing.
- Real-time dashboards showing queue depth, hold times, abandonment rates, and agent performance, not end-of-day reports.
- Customizable scorecards tied to your specific quality metrics, not generic templates.
- Trend analysis that connects call center performance to downstream outcomes: no-show rates, revenue captured, and patient satisfaction scores.
For operations leaders, building a quality assurance program is the foundation. Choose one that gives you census-level visibility, not a keyhole view.
Implementation, Support, and Scalability
The best feature set is worthless if implementation takes 18 months or breaks existing workflows. Ask:
- What is the implementation timeline? For a mid-size health system, 8-12 weeks is reasonable. If a vendor quotes 6+ months, ask why.
- Who handles integration? Some vendors hand you documentation. Others deploy engineers to configure alongside your team. That difference affects go-live success.
- What does support look like? Dedicated account managers vs. ticket queues. SLA-backed response times vs. “we’ll get back to you.”
- Can the platform scale? If you add locations, acquire practices, or face seasonal surges, does pricing and performance scale cleanly, or hit limits?
See where an AI agent fits in your operation.
Book a demoMedical Call Center Feature Comparison Matrix
Use this matrix to compare the three solution types across the criteria above. The categories are traditional telephony platforms, horizontal AI tools adapted for healthcare, and purpose-built healthcare AI platforms.
| Criterion | Traditional telephony | Horizontal AI | Healthcare-specific AI |
|---|---|---|---|
| EHR integration | Custom development | API-level, limited | Pre-built connectors (Epic, Cerner, eClinicalWorks) |
| Call analysis | 1-5% manual sample | 100% for QA | 100% plus workflow actions |
| Automation depth | Routing only | Insights and agent assist | Agentic: scheduling, eligibility, outbound |
| Compliance | BAA, stored recordings | BAA, PII redaction | BAA, zero-retention options |
| Typical deploy time | 3-6 months | 4-8 weeks | 2-6 weeks |
Ranges are illustrative and vary by organization size, call volume, and feature scope. Confirm each capability against your own stack before you buy.
Pricing Models and ROI
Medical call center pricing is often opaque. Focus on total cost of ownership.
Common models:
Per-seat/per-agent licensing: Works for stable teams but penalizes seasonal scaling. Watch for add-on charges for recording, analytics, or compliance features.
Per-minute or per-interaction pricing: Common with outsourced and AI-powered solutions. Predictable for variable volumes but can spike during high-demand periods.
Platform licensing with usage tiers: A base fee plus usage-based pricing above thresholds. Increasingly common and often more transparent.
Outcome-based pricing: Pricing tied to outcomes like appointments booked, calls resolved, or revenue recovered. Higher risk for the vendor, stronger alignment for you.
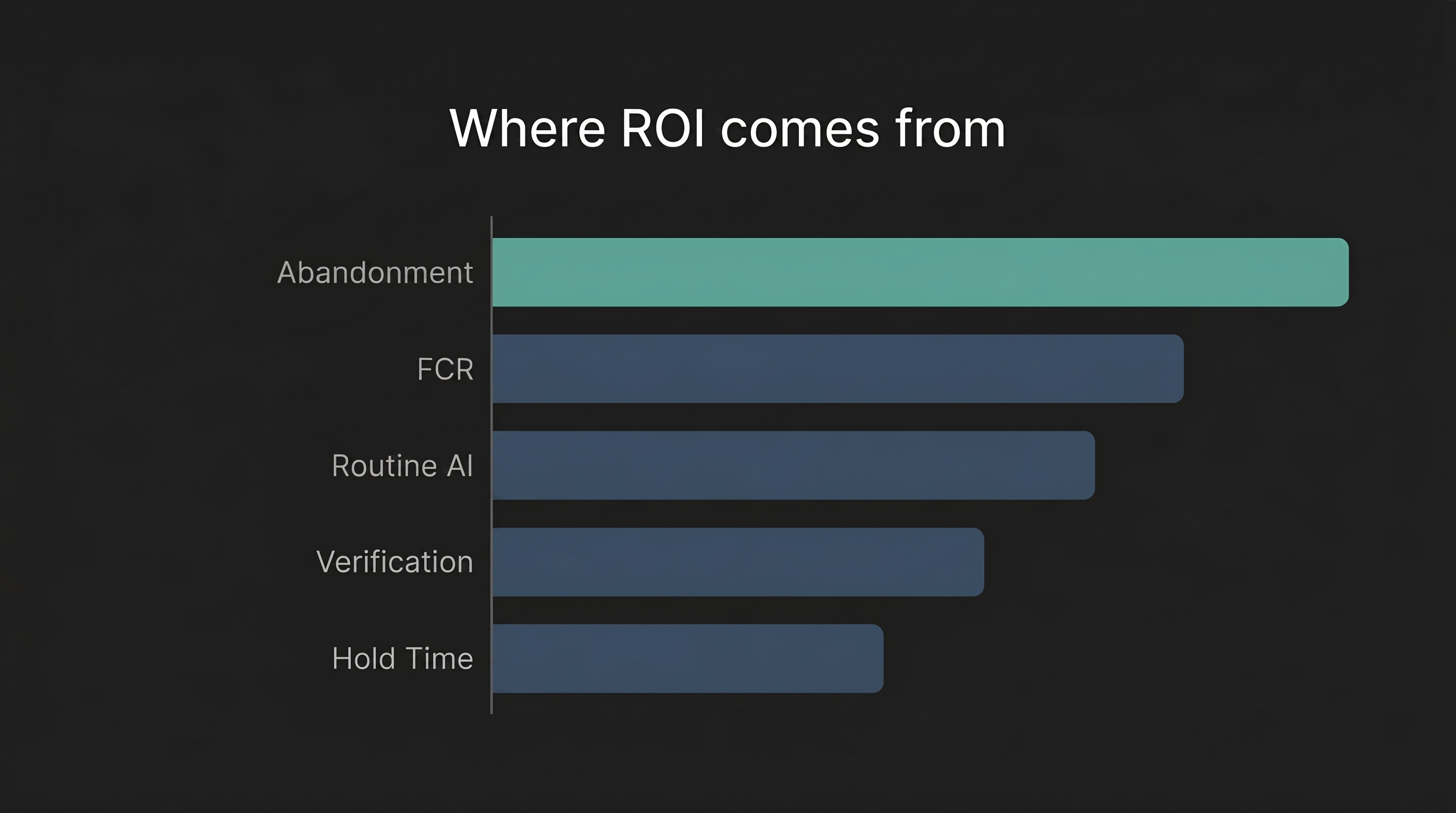
Building an ROI case:
The numbers are straightforward when you know where to look. The average healthcare call center abandonment rate is roughly 7%. On 2,000 daily calls, that is 140 abandoned calls and up to $45,000 in lost revenue per day. Reducing abandonment from 7% to 4% can recover tens of thousands of dollars per month.
The Bottom Line
The right medical call center comes down to three questions: which EHR you run and how deeply the platform integrates with it, whether you need insights or autonomous actions, and how the vendor handles HIPAA compliance and security in practice rather than on a checklist. Score each option against those, model the ROI on your own call volumes and abandonment rate, and walk away from any vendor that cannot sign a BAA or show a validated integration with your stack.
To see where your own contact center stands, request a Flexbone AI operational audit and get real call data, coverage gaps, and revenue recovery opportunities with no commitment: book a walkthrough.