A medical practice can cut front desk call volume by 50 percent or more without hiring by routing routine calls to an AI voice agent that resolves them end to end. Across primary care and specialty deployments, a well-built agent handles 50 to 70 percent of inbound volume: scheduling, reminders, refill intake, eligibility questions, and routing. The front desk keeps the calls that need clinical judgment or empathy, and the phones stop dictating the day.
This is not a staffing problem you can hire your way out of. MGMA benchmarks put medical front desk turnover near 20 percent per year, and every new hire takes 60 to 90 days to reach full productivity. The AMA has been documenting the same pattern for a decade: practices are drowning in administrative phone work while clinical time shrinks.
Most of those calls do not have to reach a human at all. A well-designed voice agent (what SEMrush still categorizes as a "medical practice answering service," only this one is AI-native) can absorb 50 to 70 percent of routine call volume on day one. Below is the math behind that claim, the playbook we use with Flexbone customers, and the specific call types you should hand off first.
Why are medical practice front desks so overwhelmed by phone calls?
Start with the volume. A typical primary care office running five providers handles 200 to 400 inbound calls per day. Specialty practices in orthopedics, dermatology, and GI often run higher because of procedure scheduling, prior authorization follow-ups, and post-op questions.
Break those calls down and a pattern appears fast. In the audits we've run (and we audit before we automate, there's a whole post on why), roughly 60-80% of inbound volume falls into the same six buckets:
- Appointment scheduling, rescheduling, and cancellations, typically the single largest category we see.
- Appointment and procedure reminders or confirmations, usually outbound and straightforward to automate.
- Prescription refill requests that get routed to the right provider or pharmacy.
- Insurance and eligibility questions patients ask before a visit.
- Billing and balance questions that rarely need clinical input.
- Routing requests, the "I need to talk to Dr. Smith's nurse" calls.
None of those are clinical judgment calls. None of them require a human ear. But every one of them pulls a trained front desk staff member off the patient standing in front of them, away from the intake paperwork, away from the copay conversation that actually needs empathy.
Layer in the human factor, MGMA's annual workforce polls have shown medical front-desk turnover hovering around 20% per year, with some practices reporting 30%+, and you get a predictable failure mode: the phones get triaged last, patient satisfaction drops, and the practice starts losing revenue to missed scheduling opportunities. KLAS research on patient access has repeatedly found that practices lose bookable appointments when patients can't get through on the first try.
How much does a single front desk call actually cost?
Here's the math practices rarely do.
Take one front desk coordinator earning a fully loaded cost of roughly $52,000/year (base + benefits + payroll tax, in line with MGMA compensation benchmarks). That's about $25/hour fully loaded.
If that coordinator spends 5 hours of an 8-hour day on the phone, and averages 4 minutes per call (inclusive of hold, after-call work, and interruptions), they handle about 75 calls/day. The fully-loaded cost per call is roughly:
- $25/hour × 5 hours = $125/day of phone labor
- $125 ÷ 75 calls = $1.67 per call
Now multiply by your actual volume:
| Daily call volume | Annual phone labor cost |
|---|---|
| 150 calls/day | ~$62,500 |
| 300 calls/day | ~$125,000 |
| 500 calls/day | ~$208,000 |
And that's just the labor on the phones. It doesn't include the downstream cost of the call, the missed appointment when the patient couldn't get through, the denied claim because eligibility wasn't checked, the no-show because the confirmation never happened. Physicians and their staff spend an average of 13 hours per week on prior authorization alone, per AMA survey data, and front-desk phone work compounds on top of that. Every unanswered call is also a lost booking, a skipped verification, or a denial waiting to happen.
What percentage of medical office phone calls can AI deflect?
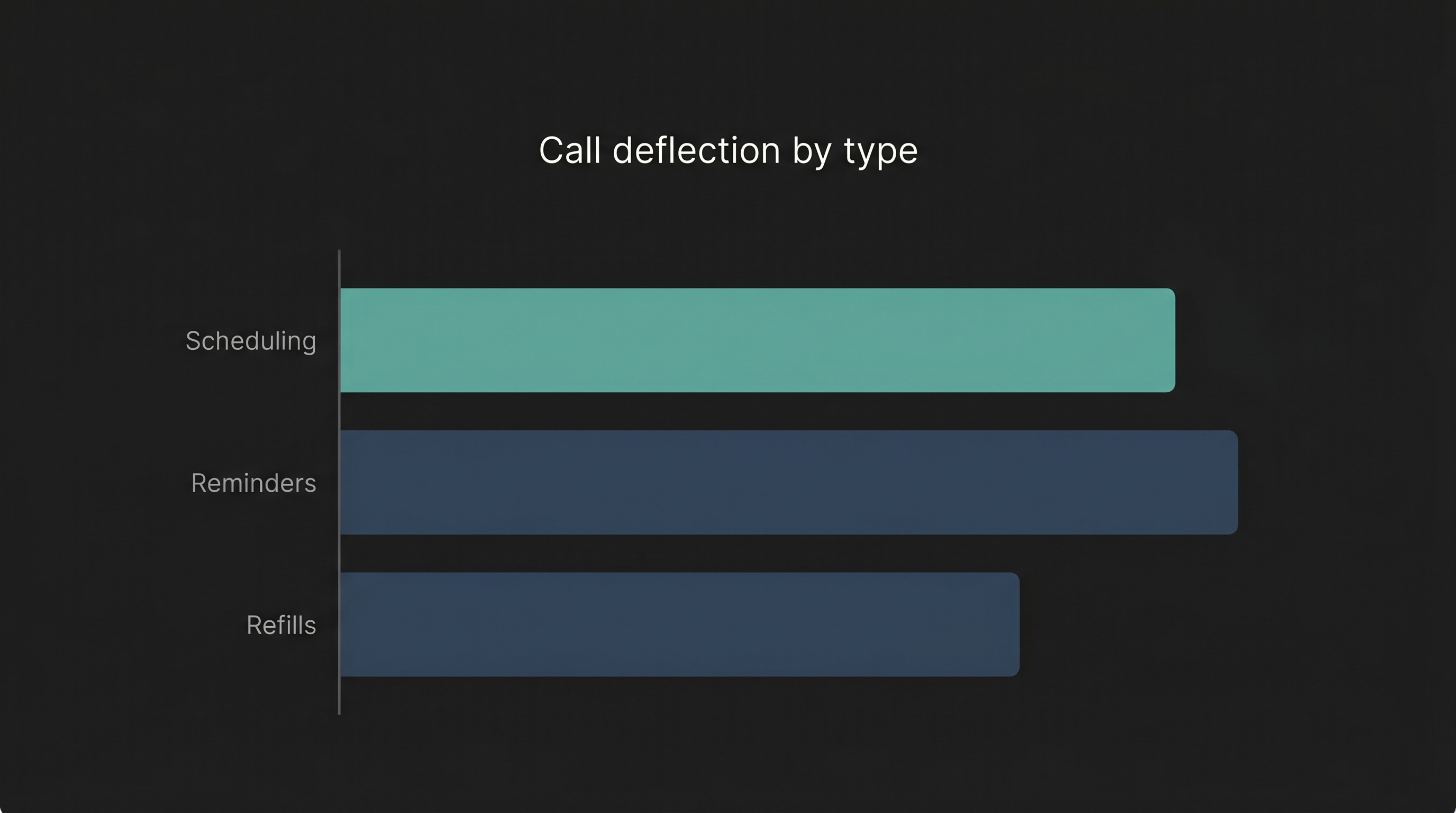
Based on Flexbone deployments across primary care, orthopedic, dental, and surgery center practices, here's a realistic deflection range by call type:
| Call type | Share of volume | Deflection rate with voice AI |
|---|---|---|
| Appointment scheduling / reschedule / cancel | 25-35% | 80-90% |
| Reminders & confirmations (outbound/inbound) | 10-20% | 95%+ |
| Prescription refill requests | 8-15% | 70-85% |
| Insurance / eligibility questions | 8-12% | 60-75% |
| Billing / balance questions | 10-15% | 50-70% |
| Routing / nurse line / general info | 10-15% | 70-85% |
| Clinical triage / complex medical | 5-10% | 0%, escalate to clinical staff |
Blend those together and the weighted average lands between 50% and 70% of total inbound volume that a modern voice agent can resolve end-to-end without touching a human. That's not a vendor promise. It's what the math produces when you multiply volume share by realistic deflection rates.
The key word is resolve. A voicemail box does not resolve anything, and an IVR that collects a callback number does not resolve anything either. A voice agent that checks the schedule, offers three open slots, books the appointment, writes it to the EHR (Epic, athenahealth, or eClinicalWorks), sends the confirmation, and flags the chart for a 270/271 eligibility check, that is resolution. That is what we build on the Flexbone Healthcare Calls platform, inside a HIPAA-compliant boundary.
The math: how to reduce front desk call volume by 50%
Let's put it together for a practice running 300 calls/day.
Before voice AI:
- 300 calls/day × 4 minutes = 1,200 minutes = 20 hours/day of phone labor
- At $25/hour fully loaded: ~$500/day, ~$125,000/year in phone labor
- 2-3 FTE effectively dedicated to phones
After voice AI (assume 55% deflection, the conservative midpoint):
- 165 calls/day handled end-to-end by the voice agent
- 135 calls/day routed to humans, averaging 4 minutes = 540 minutes = 9 hours/day
- Phone labor:
$225/day, **$56,250/year**, a ~$68,750/year reduction - The same staff now have 11 hours/day back for lobby, intake, eligibility, prior auth, and follow-up work
That is a 50%+ reduction in front desk call volume without eliminating a single role. In every deployment we've done, the practices that win biggest don't lay people off, they redeploy. The front desk coordinator stops being a switchboard and starts being the person who actually helps the patient standing in front of them. The billing lead gets the 3 hours a day they needed to work denials. The nurse line stops taking refill calls and starts taking clinical calls.
And because the voice agent writes every interaction back to the EHR and the practice management system, the downstream clean-up, missed confirmations, unchecked eligibility, unlogged refills, drops at the same time. That's the compounding effect our AI Patient Coordinator is designed to produce.
See where an AI agent fits in your operation.
Book a demoWhich calls should a medical practice answering service handle first?
In week-one deployments, we start with the highest-volume, lowest-risk call types. The sequence below is the one we use on nearly every engagement.
1. Outbound appointment reminders and confirmations. Zero deflection risk, these are calls your team is making anyway. The voice agent handles them at scale, captures confirmations and reschedule requests, and writes the result to the EHR. Practices in our deployments see a 20-30% drop in no-shows within 30 days. (There's a separate post coming on no-show reduction math, but the reminder workflow alone usually pays for the whole deployment.)
2. Inbound scheduling and rescheduling. This is the highest-volume inbound category and the one patients most want self-service on. The agent reads your real schedule, respects your provider rules, and books straight into the EHR. The AI Patient Coordinator page walks through exactly how the scheduling logic works.
3. Prescription refill intake. The agent verifies the patient, captures the medication and pharmacy, and posts a structured refill task to the clinical team, no transcription, no voicemail guesswork. Average handle time drops to under 90 seconds.
4. Eligibility and insurance questions. This is where voice AI starts pulling its weight in RCM. The agent can check eligibility in real time, tell the patient what their plan covers, and flag the chart for the billing team if anything looks off. For a deep dive on how voice connects to the rest of the revenue cycle, see our HST pathways page.
5. Routing and nurse line. The agent can answer the "what are your hours," "do you take my insurance," and "I need Dr. Smith's nurse" calls without a human ever touching them, and do it with a warm, on-brand voice, not a phone tree.
What we don't automate on day one: clinical triage, complex billing disputes, and anything emotionally loaded. Those get fast-routed to the right human with full context, the agent's transcript, the patient's chart, and the reason for the call all surfaced in one screen through our Voice Room console.
How does an AI voice agent compare to a traditional medical answering service?
A traditional answering service is, functionally, a human call center that writes down messages and forwards them. It solves the "we need someone to pick up after hours" problem, but it doesn't actually reduce your front desk workload, it just delays it. Every message still has to be worked the next morning.
A modern voice agent resolves the call.
| Capability | Traditional answering service | Voice AI agent |
|---|---|---|
| Picks up 24/7 | Yes | Yes |
| Books appointments in your EHR | No (takes a message) | Yes |
| Handles refill requests | No (takes a message) | Yes |
| Checks eligibility | No | Yes |
| Writes structured data to EHR/PMS | No | Yes |
| Scales with call volume | Linear (more agents = more cost) | Flat |
| Per-minute cost | $0.80-$2.00+ | $0.10-$0.30 |
| Patient experience | Inconsistent, often offshore | Consistent, on-brand voice |
The economics aren't close. For a 300-call/day practice, the traditional answering service route runs $50,000-$120,000/year and still leaves you with a morning queue of message slips. A voice agent runs a fraction of that and leaves you with a clean EHR.
For a broader breakdown of how voice automation fits into the rest of the phone stack, see our healthcare phone automation guide.
What does a 50% call deflection look like in practice?
A real example from a multi-site orthopedic group we worked with (details anonymized).
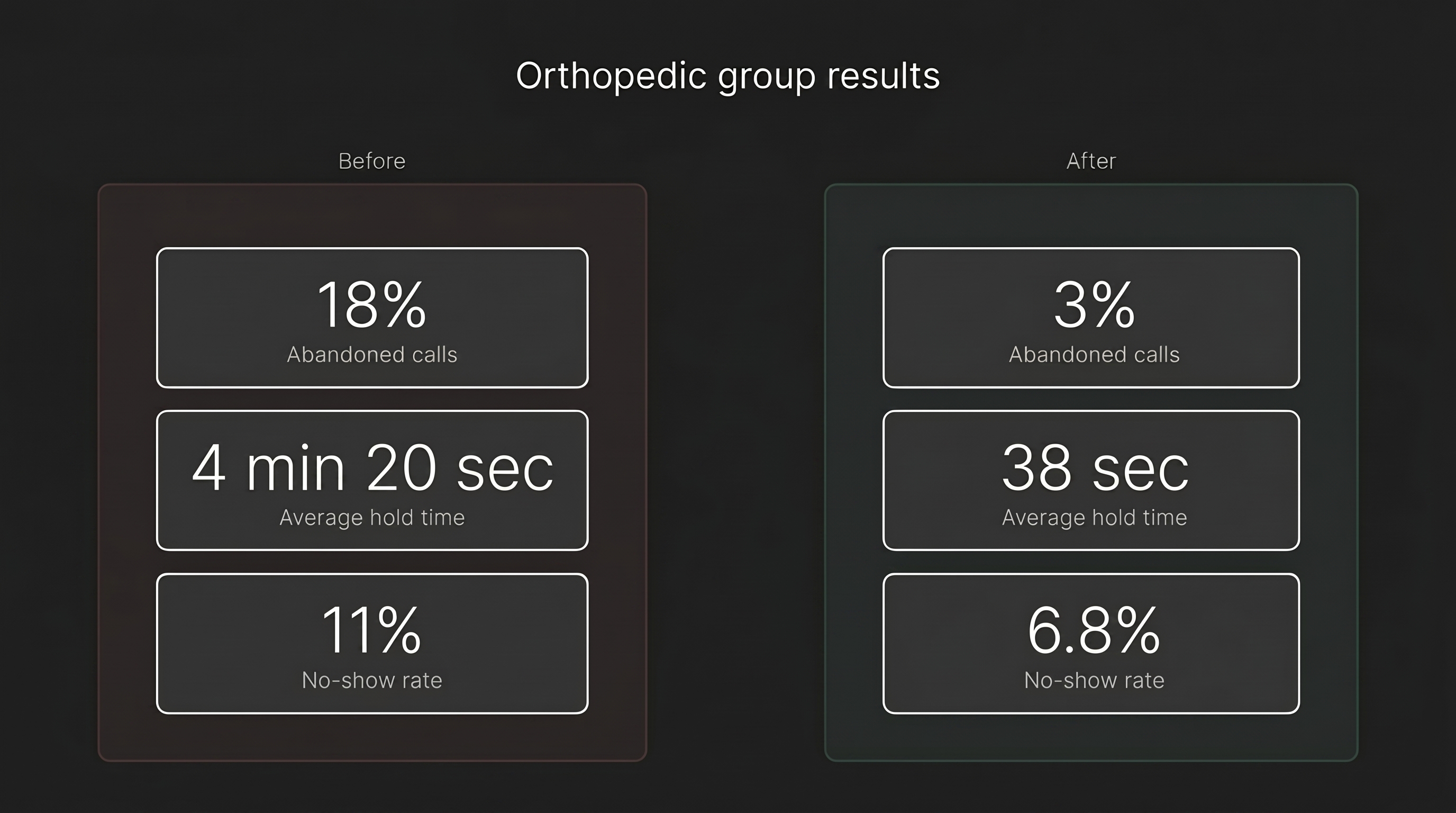
Baseline (pre-deployment audit):
- 6 sites, 28 providers
- 1,850 inbound calls/day across the group
- Average hold time: 4 minutes 20 seconds
- Abandoned call rate: 18%
- 7.2 FTE effectively dedicated to phones
- Estimated no-show rate: 11%
Four weeks after deployment of the Flexbone voice agent:
- Voice agent handling 61% of inbound volume end-to-end
- Average hold time for human-routed calls: 38 seconds
- Abandoned call rate: 3%
- Same 7.2 FTE, 4.1 redeployed to eligibility, prior auth, and in-person intake
- No-show rate: 6.8%
The practice didn't hire. It didn't fire. It stopped losing the 18% of callers who used to hang up before anyone answered, and those recovered calls turned into bookable appointments, which is where the real revenue story lives.
How to roll out voice AI without breaking patient trust
This is the part most vendors skip, and it's the part that decides whether a deployment works.
Audit before you automate. Before we change a single call flow, we listen. We classify each call category, time each workflow, and map each system the front desk touches. You can't deflect 50% of volume if you don't know which 50%.
Start with the boring calls. Reminders, confirmations, simple reschedules. Build patient familiarity with the voice before you ask it to do anything harder.
Give patients a graceful out. Every Flexbone voice agent routes to a human the moment the patient asks, the moment the conversation gets emotional, and the moment any clinical language appears. Trust is built on the escape hatch.
Write everything back. A voice agent that doesn't update the EHR and PMS is creating a second source of truth and a second problem. The write-back is where the ROI compounds.
Measure weekly, not quarterly. Deflection rate, containment rate, average handle time, no-show rate, first-call resolution, CSAT. If your vendor can't show you those numbers in a dashboard, they're selling you a phone tree with a nicer voice.
The bottom line
Front desk call overload is not a staffing problem. It's a workflow problem, and it's solvable with today's voice AI, not next year's. A correctly deployed voice agent absorbs 50-70% of routine inbound calls, gives your existing team their day back, and stops the slow revenue leak from abandoned calls and missed confirmations.
If you want to see what that looks like for your specific call mix, the Flexbone audit is the place to start. We'll connect to your phone system, classify a week of real calls, and show you the exact deflection math for your practice.
Book an audit or read more about the underlying platform on our Healthcare Calls page.